Courses & Services

Courses
The Coding Nurse® offers a variety of courses that will help get you get positioned in your new career.
ICD-10-CM
Master diagnosis coding
This foundational coding course will teach you inpatient/outpatient coding and reimbursement methodologies.
$1,499
- Introductory to Advanced Diagnosis Coding
- Coding Conventions
- Coding Guidelines
- Reimbursement Methodology (MS-DRGs/APR-DRGs)
- Overview of Outpatient Prospective Payment Systems
- Overview of Inpatient Prospective Payment Systems.
- Eligible for CRC (Certified Risk Adjustment Coder) and HCS-D (Homecare Coding Specialist - Diagnosis) coding credentials
CPT/HCPCS
Master outpatient coding
Master outpatient coding conventions, guidelines, and payment methodologies.
$1,499
- Outpatient Procedure Coding
- Coding Guidelines
- Evaluation & Management (E/M)
- Anesthesia, Surgery, Radiology, Pathology, and Medicine
- Advanced Knowledge of Modifiers
- Overview of Outpatient Prospective Payment System
CDI
Master clinical documentation review
Master clinical documentation review while optimizing facility reimbursement.
$1,499
- Use coding knowledge to make sure medical record is complete and accurate
- Learn compliant querying process
- Use knowledge of inpatient prospective payment system to optimize reimbursement for facilities
- Review of advanced ICD-10-CM coding
- Review of advanced ICD-10-PCS coding

Other Services
From tutoring to coding services—The Coding Nurse® has your back.
Tutoring
Personalized coding tutoring for exams and providers.
Tutoring sessions tailored to your learning style for exam preparation.
$40/hour
- Sessions focused on individual needs and learning style
- Perfect for exam or re-exam preparation
- Tutoring available for ICD-10-CM, ICD-10-PCS, and CPT/HCPCS code sets ($40 per hour)
- Tutoring available for billing and coding for providers ($100 per hour)
Billing & Coding
Billing support, coding audits, and instruction for providers.
Providing billing support, coding audits, & instruction for independent providers.
Inquire for Rates
- Independent billing & coding support
- One-on-One billing and coding instruction
- Specialize in CLIA Lab and mental health billing for independent providers
- Review of denied claims
- Re-submission of denied claims
- Audit of coding and clinical documentation, along with appropriate education, to enhance and streamline the revenue cycle of your business
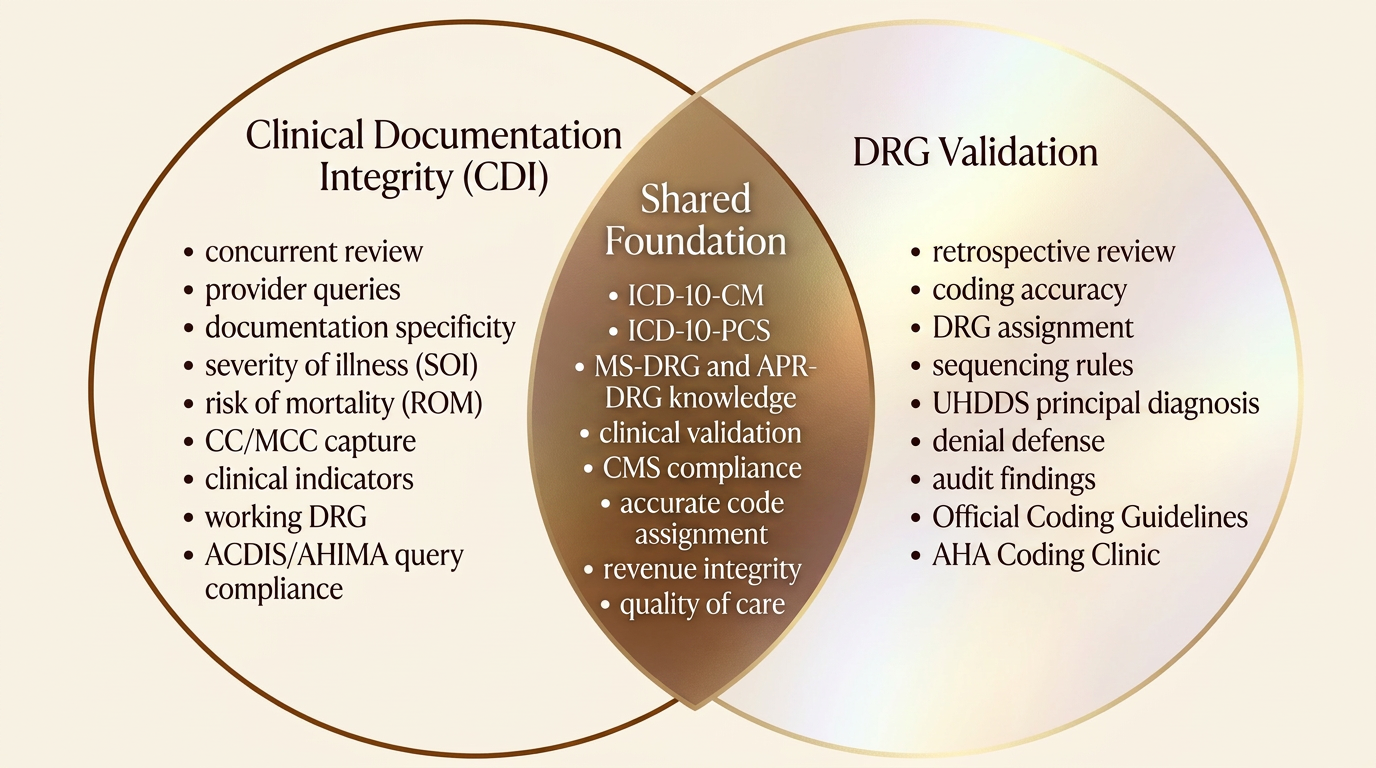
CDI and DRG Validation
Same code sets - two different roles
CDI vs. DRG Validation
| Aspect | Clinical Documentation Integrity (CDI) | DRG Validation |
|---|---|---|
| Primary Purpose | Improve the quality, accuracy, and completeness of clinical documentation in the medical record. | Verify that the assigned DRG accurately reflects the documentation and coding after the chart is finalized. |
| Timing of Review | Concurrent — typically while the patient is still admitted. | Retrospective — after discharge, coding, and billing (often pre-bill or post-bill audit). |
| Goal | Ensure documentation supports the highest level of specificity for diagnoses, procedures, severity of illness (SOI), and risk of mortality (ROM). | Confirm coding accuracy, sequencing, and DRG assignment; identify over-coding, under-coding, or unsupported codes. |
| Primary Customer | Physicians and clinical staff. | Coding department, compliance, payers, and revenue integrity. |
| Interaction with Providers | High — issues compliant queries to clarify ambiguous, conflicting, or incomplete documentation. | Low to none — typically does not query providers; communicates findings to coders or auditors. |
| Focus within ICD-10-CM/PCS | Capturing all reportable conditions, ensuring diagnoses are documented with required specificity (acuity, type, linkage, POA status). | Validating that codes assigned match documentation, follow Official Coding Guidelines, AHA Coding Clinic, and proper sequencing rules. |
| Impact on Principal Diagnosis | Influences which condition can be supported as PDx through clarification of provider intent. | Determines whether the selected PDx meets UHDDS definition and is properly sequenced. |
| CC/MCC Considerations | Identifies opportunities for providers to document conditions that may qualify as CCs/MCCs. | Validates that reported CCs/MCCs are clinically supported and correctly coded. |
| Use of Clinical Indicators | Reviews labs, vitals, meds, and treatment to identify documentation gaps and trigger queries. | Reviews clinical indicators to confirm a coded diagnosis is clinically valid (e.g., sepsis, AKI, malnutrition, respiratory failure). |
| Output / Deliverable | Provider queries, documentation recommendations, working DRG. | DRG change recommendations, audit findings, denial defense, rebill or correction requests. |
| Regulatory / Compliance Lens | Follows ACDIS/AHIMA query practice briefs; ensures queries are compliant and non-leading. | Follows Official Coding Guidelines, Coding Clinic, UHDDS, CMS rules; often defends against payer DRG downgrades. |
| Typical Background | RN, LPN, MD, or experienced coder with clinical knowledge. | Experienced inpatient coder (CCS) with strong knowledge of MS-DRG / APR-DRG grouping logic. |
| Common Credentials | CCDS, CDIP, CCDS-O, CIC, CCS. | CCS, CIC, CCDS (sometimes), CDIP. |
| Metrics of Success | Query rate, query response / agreement rate, CMI impact, SOI/ROM capture. | DRG change rate, accuracy rate, dollars recovered / protected, denial overturn rate. |
| Relationship to the Other Role | Sets the stage — better documentation upstream reduces DRG validation issues downstream. | Acts as a quality check — findings often feed back into CDI education and process improvement. |